When a horse takes an off step, the ripple of worry that follows is universal among owners. A horse’s lameness can jeopardize its career, its comfort, and sometimes its life. But pinpointing the exact source of that lameness has always been a challenge. They communicate through gait changes, behaviour, and subtle physical signs. For veterinarians, deciphering those signals often requires advanced imaging technologies that allow them to see inside the horse’s body. After a good preliminary lameness workup, it may be determined that some form of imaging is necessary to understand the type and scope of the problem.
At King Animal Hospital in King City, Ontario, Dr. Darryl Bonder, DVM, Chief Medical Officer of the hospital’s equine division, has built a career on using the latest diagnostic tools to solve equine mysteries. “It’s detective work,” he explains. “You start with the basics — history, clinical exam, nerve blocks, radiographs. But when the picture isn’t clear, you need the right imaging modality to tell you what’s really going on.”
Today’s equine veterinarians have an arsenal of technologies at their disposal, each with its own strengths and limitations. Here, Dr. Bonder explains the five main imaging modalities: ultrasound, radiography (X-ray), computed tomography (CT), magnetic resonance imaging (MRI), and nuclear scintigraphy, including how they work, when they’re used, and what they reveal.
THE FIRST STEP: BUILDING A DIAGNOSTIC ROADMAP
Before a horse ever enters an imaging suite, veterinarians rely on careful observation and hands-on tests. The process often starts with regional anesthesia — nerve blocks that help localize the source of pain. For example, if a horse blocks sound to a palmar digital nerve block, the pain originates in the foot. If the foot X-rays look clean but the lameness persists, the next question becomes: which imaging tool will reveal the hidden culprit?
“It’s all about logic,” says Dr. Bonder. “If you know the pain is coming from the foot, you don’t need to bone-scan the whole horse with nuclear scintigraphy. You decide whether the problem is more likely bone or soft tissue, and that points you toward CT or MRI. Each modality gives us a different type of information and has its advantages and disadvantages.
ULTRASOUND: THE SOUND OF SOFT TISSUE
HOW IT WORKS
Ultrasound harnesses high-frequency sound waves. The probe sends pulses into tissue, and echoes bounce back to create a real-time image. Unlike X-rays, which are best for bone, ultrasound excels at imaging soft tissue structures.
 WHEN TO USE IT
WHEN TO USE IT
- Tendon injuries: The classic “bowed tendon” is ideally evaluated by ultrasound. Vets can measure the size of the tear, assess the fiber alignment, and monitor healing over time.
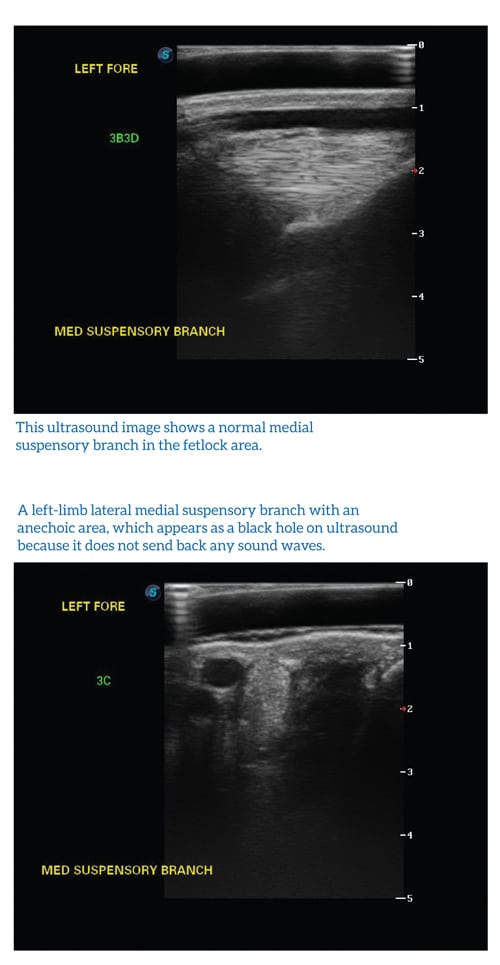
- Ligament damage: The suspensory ligament body, suspensory branches, and collateral ligaments can be visualized, often when sensitivity to palpation with or without swelling points to a specific site.
- Joint capsules and injections: Ultrasound can guide needles into sacroiliac joints or other deep structures with accuracy.
- Internal organs: From reproductive tract evaluations to echocardiograms, ultrasound has broader applications beyond lameness.
ADVANTAGES AND LIMITATIONS
Ultrasound is portable, affordable, and noninvasive, making it a workhorse tool for ambulatory vets. But its penetration is limited. A deep soft tissue tear in the hindquarters may be difficult to visualize because the dense tissue scatters the sound waves. Similarly, pelvic injuries are largely out of reach.
A CLOSER LOOK
Dr. Bonder describes how ultrasound distinguishes between different types of tissue changes. An “anechoic” black area might represent a fresh hematoma or fluid pocket, while a “hyperechoic” bright white zone could indicate scar tissue. By rotating the probe and capturing both cross-sectional and longitudinal views, vets build a complete picture of the injury. “It’s not just about spotting a lesion,” he notes. “We measure how long the tear is, how much of the tendon cross-section is affected, echogenicity and how the fibers are aligned. That tells us how serious the injury is and what the prognosis looks like.”
RADIOGRAPHY (X-RAY): THE FIRST LINE OF DEFENSE
HOW IT WORKS
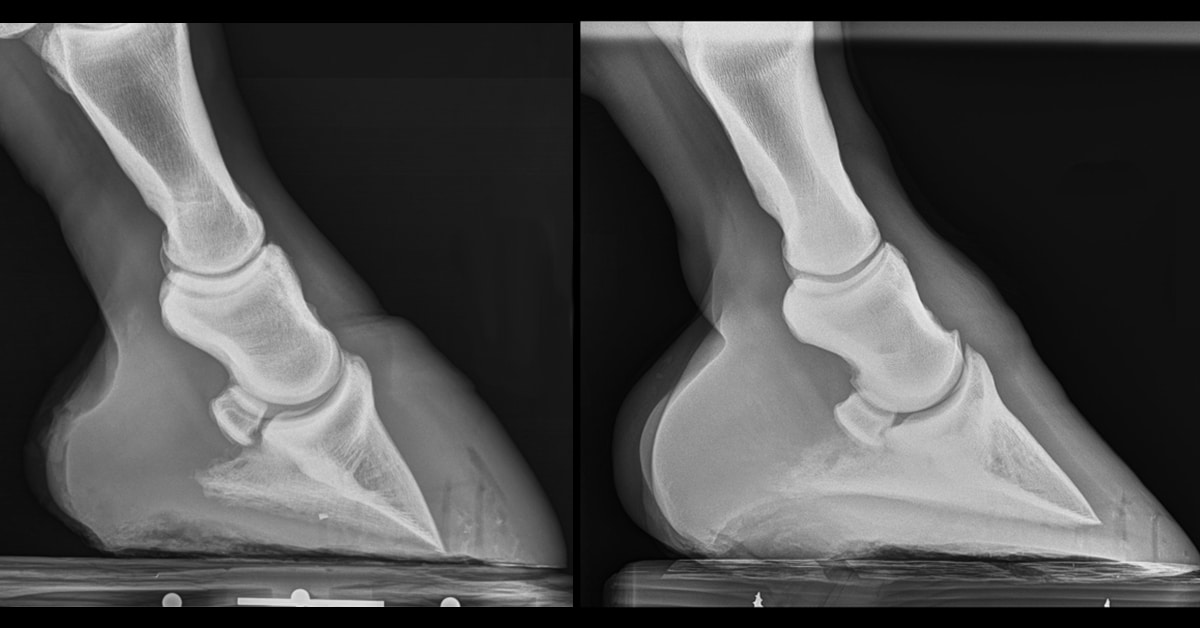
X-rays pass through the body and are absorbed differently by bone versus soft tissue and can be taken with varying intensity to get greater penetration as necessary. The result is a two-dimensional image showing fractures, chips, and other skeletal abnormalities. With digital radiography, images appear instantly and can be manipulated for contrast and detail.
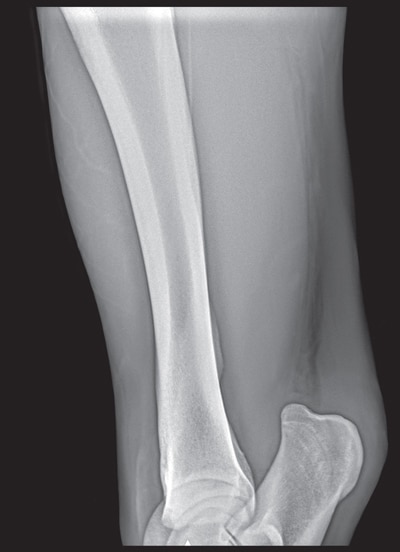
This X-ray shows some periosteal reaction – a thickening in the bone’s appearance – but does not reflect the severity of the fracture, which is seen in the nuclear scintigraphy scan below.
“X-rays are an extremely useful modality, not only in hospital, but for the ambulatory veterinarians and they have evolved tremendously,” noted Dr. Bonder, adding that digital radiography has evolved significantly so that images can be reviewed on the spot. “Having real time imaging is a huge advantage, because if we see something suspicious at a specific angle, we can alter that angle to try to enhance what we’re thinking might be the pathology.”
WHEN TO USE IT
- Acute injuries: Sudden lameness with obvious swelling of a specific area.
- Localizing lameness: After nerve blocks isolate pain to a region, radiographs are often the first imaging step.
- Bone evaluation: Hairline fractures, arthritic changes, developmental pathology such as OCD, and joint chips are all visible on X-ray.
ADVANTAGES AND LIMITATIONS
X-rays are quick, accessible, and inexpensive compared to advanced imaging. They’re the logical first step when bone injury is suspected. They show surfaces and overlapping shadows — not internal bone architecture or soft tissue in detail. A perfectly normal-looking radiograph doesn’t always mean there is no pathology. For example, a lame horse that has been blocked sound to an ankle region but has “clean” X-rays are situations where you might escalate to a CT or MRI.
COMPUTED TOMOGRAPHY – (CT): SLICING THROUGH THE DETAILS
HOW IT WORKS
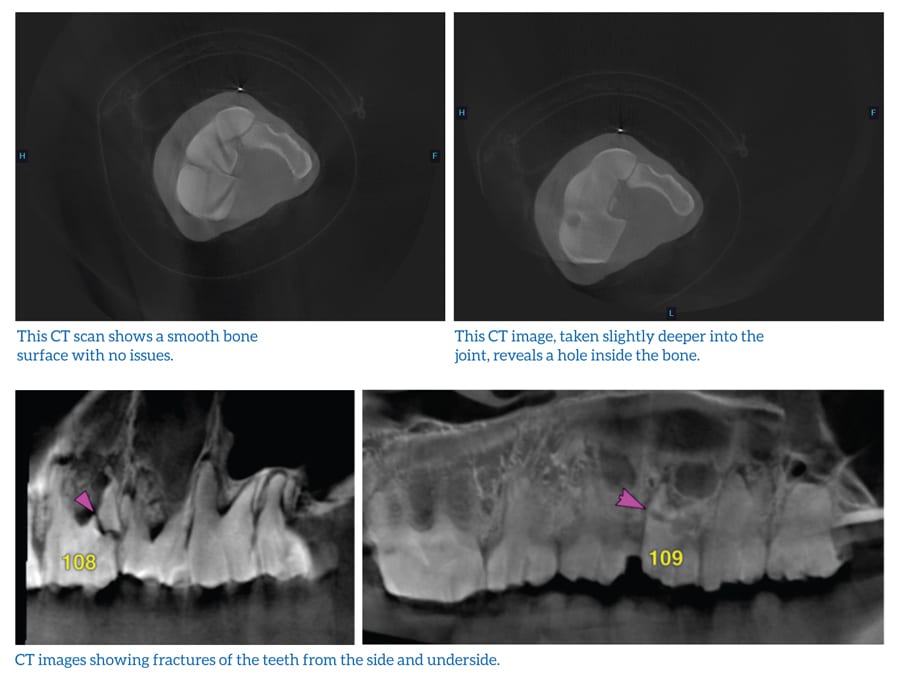
CT scans use rotating X-ray beams and computer algorithms to create cross-sectional images of the body. These “slices” can be reconstructed into 3D models, allowing vets to examine internal structures layer by layer.
WHEN TO USE IT
- Hidden bone lesions: Subtle cysts, bone edema, or stress fractures invisible on standard X-ray.
- Complex fractures: Especially spiral fractures of long bones, where surgical planning requires exact
orientation. - Detailed joint assessment: Carpal, fetlock, and foot imaging with extraordinary precision.
ADVANTAGES AND LIMITATIONS
CT is fast — a standing robotic CT unit can scan a limb in minutes without anesthesia. The ability to rotate, magnify, and contrast images gives surgeons an invaluable roadmap when planning for internal fixation. However, CT struggles with massive areas like the pelvis or thorax, where penetration is insufficient.
In the case illustrated above, an X-ray of the horse’s tibia (bone above the hock) appeared normal but the CT scan revealed a cyst-like hole inside the bone, complete with a sclerotic rim. “That’s something you’d never see on an x-ray,” Bonder explains. “It was entirely inside the bone with normal bone superimposed over the cyst. Without CT, we would have missed it.”
For orthopedic surgeons, CT is indispensable. Knowing the exact angle of a spiraling fracture determines where to place screws and plates. “You want your fixation perpendicular to the fracture line,” says Bonder. “CT shows us exactly where that line travels.”
MAGNETIC RESONANCE IMAGING (MRI): THE GOLD STANDARD FOR SOFT TISSUE
HOW IT WORKS
MRI relies on powerful magnetic fields and radio waves to detect signals from hydrogen atoms in tissues. Different imaging sequences emphasize either bone or soft tissue, producing exquisitely detailed slices through the limb or head.
WHEN TO USE IT
- Foot lameness: The foot of the horse is a highly complex structure with many types of tissue that can be injured. Navicular syndrome, deep digital flexor tendon injuries, navicular bursitis or distal impar ligament damage are all different structures, but will all show pain emanating from the back third of the foot.
- Soft tissue and bone together: Unlike CT, MRI captures both with high resolution.
- Head conditions: Neurologic (such as brain tumours or strokes), sinonasal (including sinusitis or cysts), or other soft tissue issues involving the eyes, ears, or dental pulp.
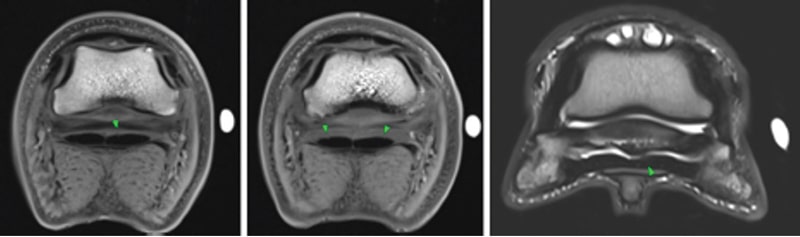
These MRI images of a hoof taken at the King Animal Hospital show the level of detail these scanners provide to better help veterinarians assess a patient.
ADVANTAGES AND LIMITATIONS
MRIs provide unparalleled detail revealing cartilage damage, subtle tendon fiber disruption, or bone bruising invisible to other modalities. Equine MRI machines are either standard (for recumbent patients) or standing. A standard MRI requires that the horse be under general anesthesia and is a lengthy process, often requiring a couple of hours. The advantage of standard MRI is its higher field strength which provides more detailed images, plus the fact the horse is not moving, compared to standing scans. There is also the risk of complications from recovery from anesthesia, but images can be taken of the head or a limb. A standing MRI is often less expensive and can be done under standing sedation and can also evaluate the distal limb.
CASE IN POINT
Bonder recalls using MRI to evaluate a horse’s foot that had eluded every other test. The MRI showed degenerative changes in the navicular region and inflammation in the deep digital flexor tendon. “It explained why the horse was painful, but nothing showed on radiograph or CT,” he says.
King Animal Hospital has two down MRIs: a 3.0 Tesla MRI used in the small animal division and
comparable to the equipment in top human hospitals. A 1.5 Tesla unit is used for equine distal limbs. “It’s extraordinary what you can see,” Bonder reflects. “But it takes time, expertise, and anesthesia, so you weigh those factors carefully.”
NUCLEAR SCINTIGRAPHY: LIGHTING UP HIDDEN INJURIES
HOW IT WORKS
Scintigraphy, often called a bone scan, uses radioactive isotopes to reveal areas of active bone turnover. A horse is injected with an isotope – technetium-99m, which incorporates into metabolically active bone. A gamma camera detects the radiation emitted, producing images that highlight “hot spots” where damaged bone is remodeling at an accelerated metabolic rate.
The timing of the scan determines which structures are highlighted as the isotope circulates through the body. Immediately after injection, the camera captures vascular images that show blood flow and can help detect clots or assess circulation in a limb. After about five minutes, the scan highlights soft tissues such as tendons and ligaments. By two to three hours, the isotope has been absorbed into the bone, which is the most useful phase in equine medicine, allowing skeletal conditions to be revealed.

This bone scan reveals a severe tibial stress fracture that was missed by the X-ray above. The highlighted area at the top is just the growth plate of young horse.
Because horses become temporarily radioactive, they remain in hospital for at least 48 hours until radiation levels drop. All horses are scanned prior to release to ensure all radioactivity has decayed to background.
“This isotope has an affinity to bone which takes up this radioactivity and incorporates it into its structure. Anywhere that there is accelerated bone metabolism, whether it be cancer, infection, fracture, the bone is turning over faster, which would result in a greater acquisition of isotope compared to surrounding tissues. The gamma camera then acts as a detector of the radiation now emitted by the horse and will highlight those areas of increased radiotracer activity during the acquisition.”
WHEN TO USE IT
- Difficult-to-image regions: Shoulders, pelvis, and spine — areas beyond the reach of radiographs, CT, or MRI.
- Multifocal lameness: Horses sore in multiple limbs, where localization is unclear.
- Poor performance: Horses that resist, refuse, or behave differently without obvious lameness. Safety cases: When blocking is risky with a fractious patient or when doing so could worsen a fracture.
ADVANTAGES AND LIMITATIONS
Scintigraphy is incredibly sensitive — it detects metabolic activity even before structural changes appear on radiographs. But it is non-specific: many findings are characteristic of an obvious condition that is easily recognized. Others may require further imaging to differentiate between inflammation, fracture or infection.
A LIFE-SAVING EXAMPLE
Bonder describes a young Thoroughbred with sudden, severe lameness. Nerve blocks risked worsening a fracture, so the horse went straight to scintigraphy. The scan revealed a tibial stress fracture — invisible on X-ray, but potentially catastrophic if missed. The horse was immediately restricted to strict stall rest. In other cases such as condylar fractures in the fetlock, lag screws can be used to stabilise the fracture. Humeral stress fractures are also potentially catastrophic. These can be identified at scintigraphy at an early stage and save lives.
COMPARING THE MODALITIES
Each imaging tool has a place in the diagnostic tree. Choosing one depends on the suspected problem, the body part involved, and practical considerations like cost and anesthesia.
Ultrasound: Best for tendons, ligaments, and guided injections. Portable and affordable.
Radiography: First-line for bone injuries; quick and inexpensive.
CT: Ideal for internal bone architecture and surgical planning; fast and detailed, but limited in depth.
MRI: The gold standard for both soft tissue and bone detail in distal limbs and head; more expensive and time-intensive.
Scintigraphy: Whole-body screening for elusive lameness; highly sensitive but less specific.

“Our job is to listen — and these tools let us listen better than ever before. Working hand-in-hand with the primary care veterinarian allows us to give the patient the best of diagnostics and treatment.” ~ Dr. Darryl Bonder, DVM
Dr. Bonder sums it up: “There’s the theoretical best — and then there’s what makes sense for that horse, at that time. Sometimes it’s about avoiding anesthesia. Sometimes it’s about cost. But the goal is always the same: to find the source of pain and guide treatment.”
LISTENING TO THE HORSE
In the end, imaging isn’t just about pictures — it’s about listening. Horses don’t act out of spite; they act out of pain. A jumper that suddenly refuses fences, or a dressage horse that resists collection, may be telling us something is wrong long before obvious lameness appears.
With today’s advanced imaging, veterinarians can honour that communication. By seeing inside the horse, they not only diagnose problems earlier, but also give horses the chance to recover fully and return to their best selves.
“The horse is always talking to us,” says Bonder. “Our job is to listen — and these tools let us listen better than ever before. Working hand-in-hand with the primary care veterinarian allows us to give the patient the best of diagnostics and treatment.”
***
This article first appeared in the 2026 Canadian Horse Annual – order your copy HERE.
The Latest