Over the past two decades, research has improved our understanding of the most common equine endocrine diseases: pituitary pars intermedia dysfunction (PPID, formerly referred to as Equine Cushing’s disease), and equine metabolic syndrome (EMS). One of the most critical new findings is that insulin dysregulation (ID) is the key driver of horses developing endocrinopathic laminitis, or now called hyperinsulinemia-associated laminitis (HAL), formerly referred to as founder. As we learn new information about these disorders, we continue to change the guidelines and recommendations for diagnostic testing. If a horse is suspected to have one of these endocrine disorders, timely and accurate diagnostic testing is key for developing a management and dietary plan to lower the risk of these horses developing laminitis. Diagnostic testing and outcomes are not a “one-size-fits-all” model, as there are different metabolic types. Thus, evaluating the complete picture, including both clinical signs of disease and diagnostic testing, is critical.
Brief Review of PPID, EMS and the involvement of ID
ID is the key feature and top concern for equids with EMS, and ID can coexist in equids with PPID. PPID is a progressive and debilitating disease affecting older horses of all breeds with a reported prevalence of more than 20% in horses older than 15 years and more than 25% in horses older than 20 years. PPID is characterized by abnormal growth and function of the pituitary gland in the pars intermedia region, causing abnormal secretion of various hormones.
This then contributes to the clinical signs seen with PPID, which can be varied and include hypertrichosis/hirsutism (overabundant hair growth and failure to shed hair), weight loss, abnormal fat redistribution, muscle wastage/atrophy, lethargy and depression, polyuria/polydipsia (increased drinking and urination) and increased susceptibility to infections such as sinusitis and hoof abscesses being most common.
Whilst most PPID cases can occur without EMS/ID being present, PPID can coexist in a subset of horses with both EMS/ID. Horses with PPID and ID will be at a higher risk for laminitis, but at this time the specific link between PPID and ID has not been fully clarified.
EMS is extremely common, with a recent study of ponies and cobs in the United Kingdom reporting a prevalence of 23%. The breeds most at risk of developing EMS include the pony breeds, Spanish breeds, gaited breeds, Morgans, miniature horses and warmbloods. These breeds have a high-genetic risk of developing EMS with only mild environmental influences, although other horses with lower genetic risk can still develop EMS if pushed by environmental factors including diet and lack of exercise. Ultimately, EMS is not a single disease but a collection of risk factors for endocrinopathic laminitis – the leading cause of laminitis. At the core of this group of risk factors is ID and generalized or regional adiposity (cresty neck and subcutaneous deposits of adipose tissue behind the shoulders and at the tail head). That being said, we now know that not all obese animals are ID. Indeed, some animals may have a lean phenotype and are considered the non-obese manifestation of EMS, while these are often horses with PPID and EMS.
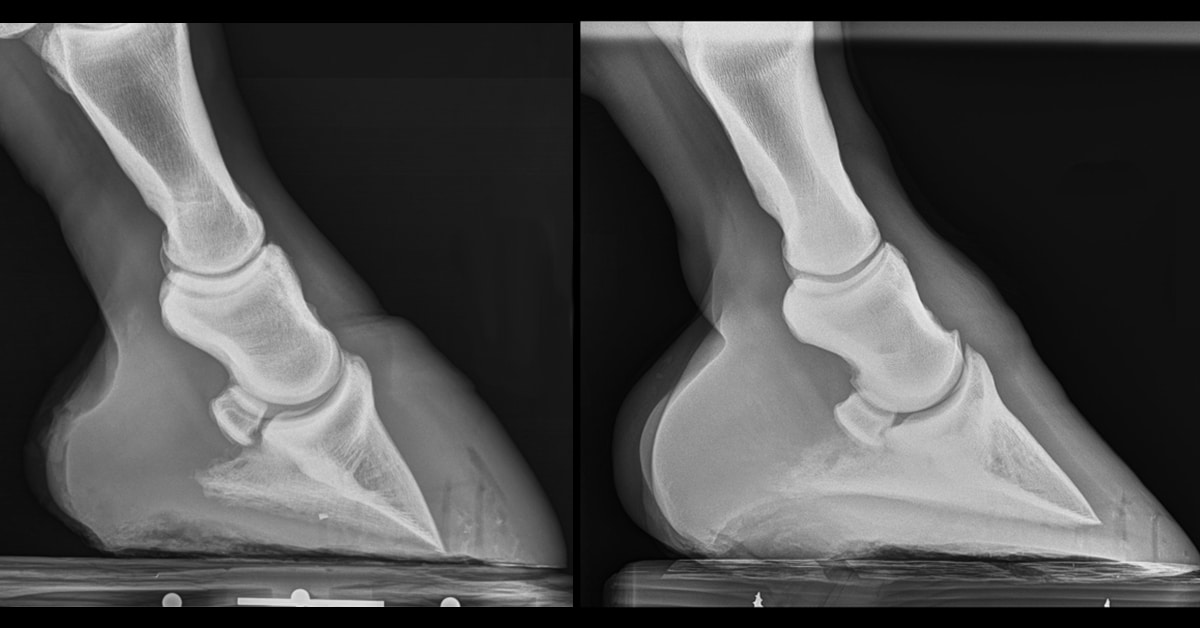
ID is characterized by an abnormal, postprandial (after feeding) metabolic response, especially with diets containing increased levels of carbohydrates. It is this abnormal insulin response that increases the risk of horses developing HAL, a painful hoof condition which often results in the need for euthanasia. While increased insulin is concerning when sustained hyperinsulinemia over ~100 uIU/mL is observed, precise cut-offs are unknown at this time. Regardless, the key to preventing laminitis is the appropriate diagnosis of ID and subsequent management changes to maintain healthy postprandial responses to diets by lowering circulating insulin responses.
How to diagnose ID?
One should incorporate diagnostic testing for ID if an equid has history or clinical signs of EMS, or if one suspects an equid to be PPID and ID. ID diagnostic testing should be considered during a wellness or pre-purchase exam, when considering corticosteroid use, or as a tool to help guide decisions with nutritional management and monitoring of an equid that has been diagnosed with ID.
ID is defined as any combination of the following: basal (resting) hyperinsulinemia, postprandial hyperinsulinemia (response to the oral sugar test or consumed feeds) or tissue insulin resistance (IR). The most accepted and practical in-field diagnostic tests for ID are measuring resting (basal) insulin and/or performing dynamic testing using the oral sugar test (OST). Measuring resting or basal insulin requires collecting a single blood sample from an equid in the fed state (hay or pasture, but not grain, which is explained further below); either plasma or serum insulin concentrations are then used to detect resting hyperinsulinemia (HI). This approach is really used for convenience sampling or monitoring, as it has a low sensitivity/high specificity, meaning it can detect more severely affected equids but does a poor job identifying mildly affected equids.
Unfortunately, resting insulin levels can be normal in some ID animals, which emphasizes the importance of dynamic testing using the OST. Resting insulin is also useful when assessing postprandial responses to a horse’s current diet regimen or monitoring responses to management changes.
The two currently recommended dynamic tests for diagnosing ID are the OST and the insulin tolerance test (ITT). The OST is preferred because the insulin response reflects the natural sequence of events that mimic the response to a meal, including digestion, absorption, hormone responses, secretion of insulin from the pancreas and risk of HAL, versus the ITT which measures hepatic and/or tissue insulin sensitivity. To conduct the OST, it is currently recommended that the equid undergo a three to six-hour fast, followed by administering either a low dose (0.15 mL/kg) or high dose (0.45 mL/kg) of lite corn syrup. Recent research characterizing the OST test has indicated a few important considerations when testing, including the fed vs fasted state of the animal prior to the OST; low vs high dose of corn syrup; season; and stress. For more information about these studies, contact Dr. Amanda Adams (Amanda.adams@uky.edu). Research has shown that winter and spring can exacerbate ID, thus one may avoid this time of year for testing or at least keep this in mind when testing during these times. Currently there are no seasonal reference ranges for diagnosing ID.
In cases where ID is thought to coexist with PPID, diagnostic testing for PPID is important. Today, the most recommended and frequently used diagnostic tests for PPID are 1) measuring baseline plasma ACTH concentrations and/or 2) measuring ACTH concentrations following the thyrotropin-releasing hormone (TRH) stimulation test, which is believed to be the most discriminating method. Determining which test is most appropriate for an individual case should be guided by clinical signs or stage of disease. If early stage is suspected, the TRH stimulation test is preferred. If moderate or advanced PPID is suspected, assessing baseline ACTH concentration may be sufficient. Retesting is recommended if results are not consistent with clinical signs. If results fall within equivocal range, the TRH stim is recommended. Given that season has an impact on ACTH levels, if possible, it’s best to avoid fall testing.
For all diagnostic testing purposes (PPID and/or ID), it is critical to send samples to a reputable lab that has established reference ranges for each of the tests. Since not all labs and assays are the same, the same facility for sample testing should be used, especially if comparing results. Additionally, consider reviewing the Equine Endocrinology Group’s published guidelines for up-to-date diagnostic testing protocols, and recommendations for reference ranges and interpretation of testing results here.
Additional information regarding the Adams’ Lab research going on at the University of Kentucky’s Aged Horse Research Center can be found at www.seniorhorsehealth.com.
~ Dr. Amanda Adams, Associate Professor, Gluck Equine Research Center
The Latest